Pathways to a Healthy Kansas is the largest community grant program funded by Blue Cross Blue Shield Kansas. The Pathways program was established in order to provide community coalitions the resources they need to remove barriers to health and engage communities to live a healthier lifestyle. Grant recipients are required to engage in a cross-sector collaboration in order to address the program’s seven focus areas in order to create sustainable change in communities. The seven areas are community policy, community well-being, food retail, health care, restaurants, schools, and worksites. The focus areas aim to promote active living, healthy eating, and tobacco prevention.
“Since 2009, Nemours FPI has been investing in disease prevention and health promotion in central Florida in an effort to address childhood obesity and promote healthy, early childhood development. Focusing on children’s first five years of life is based on the recognition that habits are still forming in the early years, early learning gives value on acquired skills, and early prevention beats the cost of later remediation. Nemours FPI has provided training and resources to central Florida child care programs including distribution of the Healthy Habits for Life Child Care Resource Kit – developed in partnership with Sesame Workshop, Nemours Health & Prevention Service and KidsHealth. Since then, working in partnership with Head Starts, Early Learning Coalitions, the University of Florida/IFAS Extension Offices, and other higher learning institutes, Nemours FPI has used a train-the-trainer model to provide healthy eating and physical activity training to child care providers, including family child care homes. Over time, FPI’s prevention and population health interventions have focused on communities in need to provide direct training and technical assistance” Nemours Florida Prevention Initiative.pdf
“The mission of the Access to Healthy Foods Research Group is to build evidence, capacity, and support for an equitable food system that fosters the health and wellness of children, families, and communities in Arkansas. The work of the ATHF Research Group focuses on the development, delivery, and evaluation of individual and environmental-level interventions such as farm to school, school and community gardens, and support for increased local and healthy food production, distribution, and consumption.”
The Community Health Program (CHAP) was founded in the 1960s to provide health care access to rural communities. CHAP is a network comprised of approximately 550 Community Health Aides/Practitioners (CHA/P)in more than 170 rural Alaska villages.
To become a CHA, members from the communities are trained in Anchorage, Bethel, Nome, and Fairbanks where they undergo an intensive program that includes classroom instruction, hands-on training, and clinical practice. The program gives the aides the skills to provide a number of services such as eye exams, responding to emergencies and diagnosing ear infection. After the program, aides go back to work in their communities to start seeing patients. The aids work closely with medical professionals in their regional hospitals. Website: http://www.akchap.org/html/about-chap.html
Dr. Lindsey is the executive director of the McSilver Institute for Poverty Policy and Research at New York University. He also leads the working group of experts supporting the Congressional Black Caucus Emergency Task Force on Black Youth Suicide and Mental Health. The Task Force report, Ring the Alarm: The Crisis of Black Youth Suicide, released in December 2019, is a comprehensive examination of the alarming rise in suicide rates for Black youth over the past generation; a survey of available data and evidence; and a call for policymakers and communities to take action to better understand and to reverse this emergent trend.[1]
TFAH: Please describe your work at the McSilver Institute.
Dr. Lindsey: We focus on the social determinants of mental health, as well as trauma and treatment disparities, all of which intersect with intergenerational poverty. If you are experiencing inequality related to, for example, food insecurity or underemployment, that has a psychological impact. We are looking for ways to break that cycle. We are committed to studying intergenerational poverty, not only to understand its consequences, but to also do something about it.
TFAH: Where does your passion for your work come from?
Dr. Lindsey: I’ve always been interested in mental health treatment disparities, particularly the lack of treatment access for serious mental health issues among Black people. I know the consequences of lack of mental health treatment. My passion derives from growing up in the Southeast section of Washington, D.C., where I saw the effects of drug use and undiagnosed, untreated addiction and mental health issues. I want to bridge that gap to make sure kids and families are connected to treatment in meaningful ways.
TFAH: If you could recommend to policymakers one or two actions that would make a real difference on the social determinants of mental health, what would they be?
Dr. Lindsey: Let’s focus that a bit. And that’s a key point. Whatever we design as an intervention has to speak to the unique issues that are experienced by a specific group. For example, looking at the rising rates of suicide among Black youth. We need to have mental health professionals in schools, proportionate to the number of kids in that school. We can’t have one provider trying to serve 500 kids or even 100 kids; that’s too many. We also need to see more federal research dollars, specifically, for studying the increasing rate of Black youth suicide. The data are clearly telling us that Black youth are at high risk.
TFAH: Does the research you are calling for need to be population-focused?
Dr. Lindsey: No question, it does. The research also needs to be gender-sensitive and culturally appropriate. We need to understand how families of color, in this case, Black families, resolve mental health challenges. For example, do we need to involve clergy in the intervention programs? Do we need services in non-traditional settings? Do we need to provide services in places other than those that the community believes are where “crazy people” go? Setting up services from the consumer perspective will help us establish services that are going to be meaningful.
TFAH: What’s the impact of the school environment on the lives of Black children? Are you concerned about school disciplinary policies that have unintended consequences for students who end up in trouble with the juvenile justice system?
Dr. Lindsey: This is something I’m particularly concerned about. For students of color, there’s implicit bias in how their behaviors are interpreted. If you have a White kid and a Black kid and a Latino kid—if the Black or Latino kid aggresses toward someone, the reaction is that kid is a bad kid, one who should be removed from school. But if a White kid acts up, he is perceived as having emotional challenges. The White kid is not suspended, he’s offered mental health services. It happens a lot.
When Black kids are suspended from school, they can be wayward in the community, they’re not engaged, their behavior comes to the attention of law enforcement—it’s a vicious cycle. It’s also tough for those same kids who are suspended from school to return to school because those school communities often don’t want them back. The largest number of students who have this lack of school engagement tend to be Black and Brown.
If we had intervened on those behaviors early on and gotten those kids to mental health treatment and associated services, we could have averted that later suspension from school. It’s a matter of how we interpret the behavioral presentations of kids. It happens to be that Black and Brown students are the ones who are not getting the requisite services surrounding their mental health.
TFAH: What has been the impact of zero-tolerance policies in schools on students of color?
Dr. Lindsey: Zero-tolerance has had a big impact on what I would call school persistence and staying connected to school among Black and Brown kids. Zero-tolerance policies do not work, and they disadvantage low-income kids and kids of color.
TFAH: McSilver’s Step Up program is established in two New York City high schools. Can you tell us more about it?
Dr. Lindsey: Step Up is focused on positive youth development. What we do is take students who are at risk for truancy or school dropout, and we wrap-around services to support them. It includes peer support—so a lot of peer-based mentoring—as well as professionally led activities to help kids stay on a positive course. The program has an 85 percent graduation rate; that’s about 10 percent higher than the general graduation rate in New York City. Programs like Step Up or school mental health services that can be offered to kids who are struggling can be very important to ensure that these kids stay connected.
TFAH: You led the expert working group that helped inform the work of the Congressional Black Caucus Emergency Task Force on Black Youth Suicide and Mental Health. What did the task force find and what did it recommend?
Dr. Lindsey: Black youth suicide and suicidal behaviors are rising. Black boys (ages 5 to 12 years old) are twice as likely to die by suicide as compared with their White peers. We led a study at the McSilver Institute that found that the self-reported suicide attempt rate for Black youth increased by 73 percent between 1991 and 2017; meanwhile, self-reported suicide attempt rates fell for White and Latino kids and for Asian and American Indian/Alaska Native kids during the same period.
What needs to be done is many of things we’ve talked about. We’re calling for mental health professionals in every school and for more National Institutes of Health funding. We’re calling for Mental Health First Aid to be widely implemented in schools. All the professionals in schools should be well-versed in the presentation of mental health issues, the signs that a student may be having trouble and how to get that student connected to supportive treatment.
We are also calling for more demonstration projects, programs that would implement evidence-based and best practices for clinicians and teachers and anyone who interacts with Black youth. We are calling for investment in demonstration projects to identify exemplars and then implement those programs at scale.
TFAH: What is required to scale up promising programs?
Dr. Lindsey: We have a program called Making Connections. In this program, we are targeting kids who have depression. The program works to reduce stigma. It is designed to help families understand what mental health treatment is all about and to address any concerns they might have about it. It’s a promising program I’d like to see delivered at scale. In order to do that, we are going to have to invest dollars in understanding how this program works. We are currently funded by NIMH [National Institute of Mental Health], but we are going to need increased funding to be able to do this in other places. If we are going to deliver these programs at scale, we are going to have to engage in the research to take them to scale. That means establishing the efficacy of programs like Making Connections, but also determining how best to implement programs like it at scale.
TFAH: Anything else you want to share?
Dr. Lindsey: I’m reminded of the power of storytelling. We need to demonstrate how implicit bias is impacting Black and Brown kids, bias that is potentially an underlying feature of why we are seeing the rising suicide trends. We need to tell the story of implicit bias in compelling ways. I believe that will challenge folks to action. It’s also important to recognize the role that stigma and mistrust play in the disconnection from services. They play a huge role in terms of the disconnection from mental health treatment. We need to work on bridging those gaps between need and use of treatment.
[1] Watson Coleman B. Ring the Alarm: The Crisis of Black Youth Suicide in America. Washington, D.C.: Congressional Black Caucus Emergency TaskForce on Black Youth Suicide and Mental Health, December 2019. https://watsoncoleman.house.gov/uploadedfiles/full_taskforce_report.pdf (accessed April 30, 2020).
(Washington, DC – May, ) Trust for America’s Health has created a new web-based tool that will allow members of Congress, their staff and grassroots health advocates to identify the health needs of constituents and target programs and resources where they are most needed.
The new web tool, How Healthy is your Congressional District? created by TFAH with data provided by the Centers for Disease Control and Prevention, is a one-year snapshot of health measures for every congressional district in all 50 states and the District of Columbia. These data were reported within the CDC’s Behavioral Risk Factor Surveillance System (BRFSS) for 2017.
Data, reported nationally, by state and by Congressional district, as part of this website are:
Percentage of adults who lack health insurance
Current percentage of adults who smoke
Cholesterol screening within the previous five years among adults
Visits to doctor for routine checkup within the past year among adults
Percentage of adults who have been diagnosed with diabetes
Percentage of adults who report their general health as fair or poor
Percentage of adults who report they could not see a doctor due to cost
Percentage of adults who have obesity
Percentage of adults who report they have no leisure-time physical activity
Percentage of adults who received a flu shot or flu vaccine during the past 12 months
Ten of the eleven indicators are measures of adults aged 18 years and older; the health insurance measure (#1) is of adults 18-64.
Data should drive policymaking. Toward that goal, TFAH is providing this data reporting tool to policymakers, community leaders, health promotion advocates, and other interested parties. The webpage provides data to policymakers and others who want to know more about the health of their congressional districts.
“Making these comparative data easily available to policymakers will help identify critical action steps and policies that if made will improve the health status of many Americans,” said John Auerbach, President and CEO of Trust for America’s Health. “These data also help identify those districts that are in the greatest need of health-promoting policy interventions”.
Why Analyze by Congressional District?
The webpage is a unique source of information on these select 11 indicators reported by the congressional district. Other existing data sources are most often available at the state or county levels. This lack of data reported at the congressional district level can make it challenging for elected officials, their staff, and local residents and organizations, to gain an accurate picture of the health concerns specific to a district.
There are health-related concerns in every district. The elevated health risk in certain districts is likely a reflection of the social, economic, and environmental conditions related to their demographic composition. These data will assist all of the residents of a district – including the elected officials – to understand what needs to be done to promote optimal health and wellbeing at the local level.
In addition, the constituents of a district may find the information useful in prioritizing their community-level efforts, when seeking resources from private and public organizations, or when tracking trends over time and when conferring with local leaders about issues of concern.
State policymakers often focus on improving residents’ health by expanding and ensuring access to quality health services. While the healthcare sector has a critical role in improving health outcomes, studies show that only 10 to 20 percent of health is determined by medical care. The circumstances in our everyday lives shape our health whether it’s where we live, how we eat, where we go to school, our workplaces, who we care for, or what opportunities we have (or don’t have) to succeed, it all has a profound effect on long-term health—regardless of what type of healthcare we receive. TFAH has developed policy briefs and resources that consider the root causes of that negatively impact public health and suggests policies that support multisector solutions, beyond the healthcare sector, to improve the nation’s health, community by community. Learn more about our work in PHACCS.
On November 18th, 2019, Trust for America’s Health held a briefing for congressional staff and partners that reviewed the latest obesity rates and trends, the role of public health and other stakeholders in preventing, treating and responding to obesity and its comorbidities, highlighted promising approaches to ensure healthy communities, and offered evidence-based policy recommendations that could help all Americans lead healthier lives.
Briefing speakers included:
John Auerbach, MBA, President and CEO, Trust for America’s Health
Devita Davison, Executive Director, FoodLab Detroit
Martha Halko, MS, RD, LD, Deputy Director of Prevention & Wellness, Cuyahoga County (Ohio) Board of Health
Ruth Petersen, MD, MPH, Director, Division of Nutrition, Physical Activity, and Obesity, Centers for Disease Control & Prevention (CDC)
Healthy eating among families and communities promotes optimal health and well-being. However, approximately three-fourths of Americans do not consume the recommended amounts of healthy foods, such as fruits and vegetables, set by the 2015-2020 Dietary Guidelines for Americans.
A healthy daily diet is linked to reduced risk for obesity, diabetes, hypertension, and other preventable chronic illnesses. But, despite efforts to promote healthy eating, communities across the U.S. continue to face barriers to accessing healthy foods.
Produce Rx
In 2012, DC Greens, a food justice non-profit located in Washington, DC, launched a pilot program called Produce Rx which began as a small-scale partnership between health care clinics and local farmer’s markets. The vision, like that of similar efforts across the country, was to increase patients’ access to fresh produce and empower them to make healthier food choices in order to manage and improve their health.
A sample prescription a doctor might provide for Produce Rx.
As part of the program, patients facing food insecurity and living with diet-related chronic disease enrolled in a six-month group nutrition class at a local health clinic, where they received monthly nutrition education and seasonal recipe demonstrations and had a check-in with a healthcare provider. Additionally, they received a “prescription” in the form of a voucher from the healthcare provider to purchase fresh produce from their local farmer’s market.
Community members who participated in the Produce Rx program showed significant improvements in health outcomes, such as lower BMI among 50 percent of the participants. In addition, 85 percent of the program participants reported improved patient-provider relationships.
Expansion and Growth
In March 2019, DC Greens, with funding support from the DC Department of Health and AmeriHealth Caritas, the largest Medicaid managed care organization in the District with more than 100,000 members, established a new partnership with Giant Food – the only grocery store located in D.C.’s Ward 8. The Ward 8 neighborhood has some of the highest income, educational, health, and racial and ethnic disparities among all of the District’s 8 wards – creating an opportunity to support D.C. residents with the greatest need through a new expanded model of the Produce Rx program.
D.C.’s Ward 8 is known as a “food desert” due to the limited number of retailers selling fresh, affordable produce, and the fact that the community faces disproportionate rates of people with diet-related chronic conditions. Moreover, Ward 8 has the highest rates of death due to diabetes and heart disease within the city.
“There is a myth that people living in poverty don’t want healthy food. We know this isn’t true,” says Lauren Shweder Biel, Executive Director of DC Greens. “people simply lack the resources to get the healthy foods that they want and that they need. With Produce Rx, we’ve been able to give patients a way to follow their doctors’ medical advice.”
“Giant Food is excited about the positive impact the Produce Rx program has had at our Alabama Avenue store,” said Ira Kress, interim President at Giant Food. ” As a food retailer, with roots in Washington, D.C. dating back 83 years, we recognize the important role we can play in the access to healthy foods and health education in our community, and this program has been a natural fit.”
With the new partnership Produce Rx participants will have access to fresh fruit and vegetables year-round. The program will expand its services to 500 AmeriHealth Medicaid participants who will receive a $20 voucher every week to purchase produce at their neighborhood Giant.
Produce Rx patient Adrienne Dove exchanges her prescription for a voucher for produce from Giant Food Pharmacy Manager Adaoma Chinweuba.
“AmeriHealth Caritas DC is committed to helping our members, especially those with chronic health conditions, improve their overall health by adding more fruits and vegetables to their daily diet,” said Keith Maccannon, Director of Community Relations and Outreach at AmeriHealth Caritas DC. “Collaboration with community-based organizations and businesses like DC Greens and Giant Food are a key component of our strategy in this area.”
Participants in this program will also have access to personal-level nutrition education at their health clinic and through Giant’s in-store nutritionist and AmeriHealth’s nutrition and wellness programs.
“Pairing nutrition education with produce access is essential for helping our customers unlock the power of produce,” said Jillian Griffith, Giant Food in-store nutritionist. “It is one thing to be instructed by a medical provider to eat more fruits and vegetables, but it’s another to have an in-store nutritionist available to share plant-based recipe ideas or new produce pairings for traditional family favorites. I am so grateful for the opportunity to teach Produce Rx participants the role food plays in their overall health while empowering them with the “produce tools” needed to meet dietary recommendations.”
Through these services, Produce Rx is making healthy food options more affordable and accessible for both individuals and their families.
“The program has impacted me and my family because we found we are eating healthier, losing more weight, and needing less medication than we used to,” said Adrienne Dove, a participant in the program. “I count my spending to make sure I don’t go over on food, but now I can buy healthier options, like spinach and broccoli, that my son wants to try, from the grocery store right around the corner.”
Next Steps
This next iteration of Produce Rx will run for a year, allowing DC Greens to conduct a robust evaluation of its effectiveness by measuring key behavior changes, health outcomes, and tracking health care costs among program participants. Currently, DC Greens administers Produce Rx but with this evaluation they hope to build the case for scalable and sustainable investments in these programs by the healthcare system.
(From left to right) Kevin O’Donnell (Giant Food District Pharmacy Manager), Adaoma Chinweuba (Giant Food Pharmacy Manager), Adrienne Dove (Produce Rx Patient) Samir Balile (Giant Food Clinical Programs Specialist).
“We are working to integrate ‘food as medicine’ as a key component of clinical care, but we know that the only way to truly scale a program like this is to prove a return on investment for the healthcare system,” says Biel. “With AmeriHealth Caritas and DC Health at our side, we believe this program is poised to demonstrate the impact that ‘food as medicine’ can have on individual health and patient utilization of the healthcare system.”
More Investment in Policies and Programs to Support Food Access and Healthy Choices is Needed
Continued investments in local, state, and federal policies and programs are critical for improving nutrition and health, especially among low-income and underserved communities that face limited access to affordable, fresh produce. More research is needed to definitively demonstrate the impact that DC Greens Produce Rx and other innovative programs are having on health and healthcare services usage. But the preliminary findings are promising.
“With the obesity crisis getting worse, we need to have a comprehensive and multi-faceted approach to changing the conditions that make it difficult for people to eat a healthful diet. Such an approach includes initiatives like DC Produce Rx with its focus on reducing the financial barriers to accessing healthy foods as well as providing culturally and linguistically tailored educational information,” said John Auerbach, President and CEO of Trust for America’s Health.
From community-based programs that test new strategies like Produce Rx to federal programs such as the Supplemental Nutrition Assistance Program for Woman, Infants, and Children (WIC) access to nutritious, affordable foods can help communities live healthier lives. As the nation experiences growing rates of obesity and other chronic diseases, it’s important for policymakers to continue supporting innovative solutions that address the root causes of preventable disease.
Infectious diseases disrupt the lives millions of Americans every year. Fortunately, vaccines can prevent many of these diseases. Nonetheless, because the U.S. vaccination rates are lower than they should be, unnecessary illness and even death occurs.
For example, the seasonal flu causes much preventable suffering. The Centers for Disease Control and Prevention (CDC) found an estimated 80,000 people died—among them, 185 children—from seasonal flu in 2017–2018, nearly twice what is considered typical during an average flu year. In addition to the devastating health impacts, it is estimated that seasonal flu costs the nation approximately $87 billion in medical spending and lost work productivity annually.
The U.S. is currently in the midst of its worst measles outbreak in two decades, causing more than 1,000 cases. With the measles outbreak still growing, it is important to highlight the life-saving impacts of vaccines for people of all ages and take actions to ensure that vaccine use remains a common practice.
Key Findings
Vaccines have helped save up to 3 million lives per year worldwide by preventing diseases such as hepatitis B, meningitis, measles and polio. Additionally, researchers say that every dollar spent on vaccination brings back return on investment in health, economic and societal benefits in 94 low to middle income countries.
The CDC estimates that vaccination of children born between 1994 and 2018 in the U.S. will prevent 419 million illnesses, help avoid 936,000 deaths, and save nearly $1.9 trillion in total societal costs.
In 2018, the CDC reported that the percentage of children under age 2 who had not received any recommended vaccinations quadrupled since 2001.
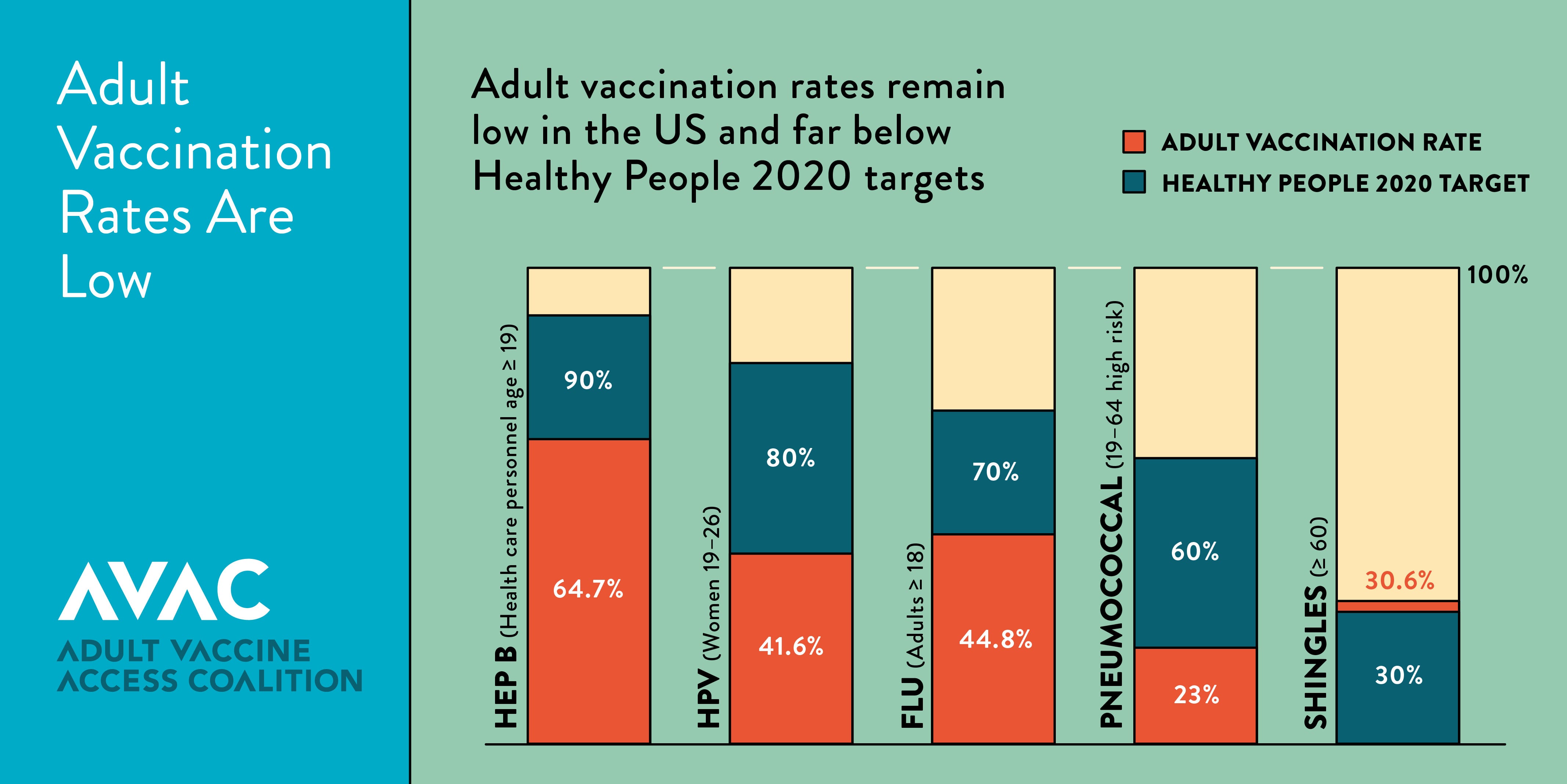
Adult vaccination rates remain far below targets in Healthy People 2020, including for hepatitis B, seasonal flu, pneumococcal, and shingles.
Seasonal flu vaccination rates for Americans ages 6 months and older dropped from 47 percent in the 2016-2017 season to 42 percent during the 2017-2018 season. The 2017– 2018 flu season in the United States was the deadliest in nearly 40 years—tragically underscoring the importance of annual vaccination.
The World Health Organization has named vaccine hesitancy, the reluctance or refusal to vaccinate despite the availability of vaccines, as one of the top ten threats to global health.
Recommendations
Significantly increase support for the vaccine infrastructure, outbreak prevention and response. CDC’s immunization program supports state and local immunization programs to increase vaccine rates among uninsured and underinsured adults and children, respond to outbreaks, educate the public and target hard-to-reach populations, improve vaccine confidence, establish partnerships, and improve information systems. Funding has not kept up with needs as states have to spend immunization dollars to respond to outbreaks, increases in the numbers of those who lack health insurance and vaccines, such as HPV, that are underused. Congress should significantly increase funding for CDC’s immunization program.
Raise awareness about the importance of vaccination and improve vaccine acceptance. Government, healthcare providers, health systems and other trusted partners should use varied and targeted media channels to educate people about the importance, effectiveness, and safety of vaccinations. Congress should provide needed resources to the United States Department of Health and Human Services to study the causes for vaccine resistance and to educate clinical providers on methods for improving vaccine acceptance.
Minimize vaccine exemptions for schoolchildren and healthcare workers. States should enact policies that enable universal childhood vaccinations to ensure children, their classmates, educators and the general public are protected from vaccine-preventable diseases. This includes eliminating non-medical exemptions and opposing legislation to expand exemptions. States should ensure medical vaccine exemptions are only given when appropriate and are not used as a de facto personal belief exemption in states where those exemptions have been eliminated. Healthcare personnel should also be required to receive all recommended vaccinations of the Advisory Committee on Immunization Practices (ACIP) in order to protect staff and patients, assure continuity of operations in the event of an outbreak and, achieve necessary healthcare infection control. Healthcare facilities should ensure access to vaccines for all staff and contractors and remove barriers for staff receiving vaccines.
Ensure first-dollar coverage for recommended vaccines under Medicaid, Medicare, and commercial insurance. Public and private payers should ensure that ACIP-recommended vaccines are fully covered, as cost-sharing can be a significant barrier to vaccination.
Increase the pool of providers who immunize. As new vaccines are approved, reaching target populations will be critical. States can expand certain health care providers’ roles and scopes of practice to increase the pool of professionals who give shots, such as pharmacists and paramedics. All insurance plans should consider including pharmacies and other complementary providers as in-network and receive equal payment for vaccine administration services for their adult and pediatric populations.







{kind=link}