Issue Category: Obesity/Chronic Disease
The State of Obesity 2019: Better Policies for a Healthier America
Produce Rx: Using Prescriptions to Improve Affordability of Healthy Foods

Healthy eating among families and communities promotes optimal health and well-being. However, approximately three-fourths of Americans do not consume the recommended amounts of healthy foods, such as fruits and vegetables, set by the 2015-2020 Dietary Guidelines for Americans.
A healthy daily diet is linked to reduced risk for obesity, diabetes, hypertension, and other preventable chronic illnesses. But, despite efforts to promote healthy eating, communities across the U.S. continue to face barriers to accessing healthy foods.
Produce Rx
In 2012, DC Greens, a food justice non-profit located in Washington, DC, launched a pilot program called Produce Rx which began as a small-scale partnership between health care clinics and local farmer’s markets. The vision, like that of similar efforts across the country, was to increase patients’ access to fresh produce and empower them to make healthier food choices in order to manage and improve their health.

As part of the program, patients facing food insecurity and living with diet-related chronic disease enrolled in a six-month group nutrition class at a local health clinic, where they received monthly nutrition education and seasonal recipe demonstrations and had a check-in with a healthcare provider. Additionally, they received a “prescription” in the form of a voucher from the healthcare provider to purchase fresh produce from their local farmer’s market.
Community members who participated in the Produce Rx program showed significant improvements in health outcomes, such as lower BMI among 50 percent of the participants. In addition, 85 percent of the program participants reported improved patient-provider relationships.
Expansion and Growth
In March 2019, DC Greens, with funding support from the DC Department of Health and AmeriHealth Caritas, the largest Medicaid managed care organization in the District with more than 100,000 members, established a new partnership with Giant Food – the only grocery store located in D.C.’s Ward 8. The Ward 8 neighborhood has some of the highest income, educational, health, and racial and ethnic disparities among all of the District’s 8 wards – creating an opportunity to support D.C. residents with the greatest need through a new expanded model of the Produce Rx program.
D.C.’s Ward 8 is known as a “food desert” due to the limited number of retailers selling fresh, affordable produce, and the fact that the community faces disproportionate rates of people with diet-related chronic conditions. Moreover, Ward 8 has the highest rates of death due to diabetes and heart disease within the city.
“There is a myth that people living in poverty don’t want healthy food. We know this isn’t true,” says Lauren Shweder Biel, Executive Director of DC Greens. “people simply lack the resources to get the healthy foods that they want and that they need. With Produce Rx, we’ve been able to give patients a way to follow their doctors’ medical advice.”
“Giant Food is excited about the positive impact the Produce Rx program has had at our Alabama Avenue store,” said Ira Kress, interim President at Giant Food. ” As a food retailer, with roots in Washington, D.C. dating back 83 years, we recognize the important role we can play in the access to healthy foods and health education in our community, and this program has been a natural fit.”
With the new partnership Produce Rx participants will have access to fresh fruit and vegetables year-round. The program will expand its services to 500 AmeriHealth Medicaid participants who will receive a $20 voucher every week to purchase produce at their neighborhood Giant.

“AmeriHealth Caritas DC is committed to helping our members, especially those with chronic health conditions, improve their overall health by adding more fruits and vegetables to their daily diet,” said Keith Maccannon, Director of Community Relations and Outreach at AmeriHealth Caritas DC. “Collaboration with community-based organizations and businesses like DC Greens and Giant Food are a key component of our strategy in this area.”
Participants in this program will also have access to personal-level nutrition education at their health clinic and through Giant’s in-store nutritionist and AmeriHealth’s nutrition and wellness programs.
“Pairing nutrition education with produce access is essential for helping our customers unlock the power of produce,” said Jillian Griffith, Giant Food in-store nutritionist. “It is one thing to be instructed by a medical provider to eat more fruits and vegetables, but it’s another to have an in-store nutritionist available to share plant-based recipe ideas or new produce pairings for traditional family favorites. I am so grateful for the opportunity to teach Produce Rx participants the role food plays in their overall health while empowering them with the “produce tools” needed to meet dietary recommendations.”
Through these services, Produce Rx is making healthy food options more affordable and accessible for both individuals and their families.
“The program has impacted me and my family because we found we are eating healthier, losing more weight, and needing less medication than we used to,” said Adrienne Dove, a participant in the program. “I count my spending to make sure I don’t go over on food, but now I can buy healthier options, like spinach and broccoli, that my son wants to try, from the grocery store right around the corner.”
Next Steps
This next iteration of Produce Rx will run for a year, allowing DC Greens to conduct a robust evaluation of its effectiveness by measuring key behavior changes, health outcomes, and tracking health care costs among program participants. Currently, DC Greens administers Produce Rx but with this evaluation they hope to build the case for scalable and sustainable investments in these programs by the healthcare system.

“We are working to integrate ‘food as medicine’ as a key component of clinical care, but we know that the only way to truly scale a program like this is to prove a return on investment for the healthcare system,” says Biel. “With AmeriHealth Caritas and DC Health at our side, we believe this program is poised to demonstrate the impact that ‘food as medicine’ can have on individual health and patient utilization of the healthcare system.”
More Investment in Policies and Programs to Support Food Access and Healthy Choices is Needed
Continued investments in local, state, and federal policies and programs are critical for improving nutrition and health, especially among low-income and underserved communities that face limited access to affordable, fresh produce. More research is needed to definitively demonstrate the impact that DC Greens Produce Rx and other innovative programs are having on health and healthcare services usage. But the preliminary findings are promising.
“With the obesity crisis getting worse, we need to have a comprehensive and multi-faceted approach to changing the conditions that make it difficult for people to eat a healthful diet. Such an approach includes initiatives like DC Produce Rx with its focus on reducing the financial barriers to accessing healthy foods as well as providing culturally and linguistically tailored educational information,” said John Auerbach, President and CEO of Trust for America’s Health.
From community-based programs that test new strategies like Produce Rx to federal programs such as the Supplemental Nutrition Assistance Program for Woman, Infants, and Children (WIC) access to nutritious, affordable foods can help communities live healthier lives. As the nation experiences growing rates of obesity and other chronic diseases, it’s important for policymakers to continue supporting innovative solutions that address the root causes of preventable disease.
The State of Obesity Report Fact Sheet (September 2019)
U.S. Obesity Rates at Historic Highs – Nine States Reach Adult Obesity Rates of 35 Percent or More
Report Calls for Sugary Drink Taxes, Expanded SNAP and WIC Nutrition Support Programs and a built environment that encourages physical activity to Help Address Health Crisis
(Washington, DC – September 12, 2019) – Nine U.S. states had adult obesity rates above 35 percent in 2018, up from seven states at that level in 2017, an historic level of obesity in the U.S., according to the 16th annual State of Obesity: Better Policies for a Healthier America report released today by the Trust for America’s Health (TFAH).
The report based in part on newly released data from the Centers for Disease Control and Prevention’s Behavioral Risk Factor Surveillance System (BRFSS), and analysis by TFAH, provides an annual snapshot of obesity rates nationwide. The State of Obesity series and this report were made possible by funding from the Robert Wood Johnson Foundation.
Obesity has serious health consequences including increased risk for type 2 diabetes, high blood pressure, stroke and many types of cancers. Obesity is estimated to increase national healthcare spending by $149 billion annually (about half of which is paid for by Medicare and Medicaid) and being overweight or obese is the most common reason young adults are ineligible for military service.
Obesity rates vary considerably between states with Mississippi and West Virginia having the highest level of adult obesity in the nation at 39.5 percent and Colorado having the lowest rate at 23.0 percent.
For the first time, adult obesity rates were above 35 percent in nine states in 2018: Alabama, Arkansas, Iowa, Kentucky, Louisiana, Mississippi, Missouri, North Dakota and West Virginia.
As recently as 2012, no state had an adult obesity rate over 35 percent and within the last five years (2013 and 2018) 33 states had statistically significant increases in their rates of adult obesity.
“These latest data shout that our national obesity crisis is getting worse,” said John Auerbach, President and CEO of Trust for America’s Health. “They tell us that almost 50 years into the upward curve of obesity rates we haven’t yet found the right mix of programs to stop the epidemic. Isolated programs and calls for life-style changes aren’t enough. Instead, our report highlights the fundamental changes that are needed in the social and economic conditions that make it challenging for people to eat healthy foods and get sufficient exercise.”
Differential Impact Amongst Minority Populations
The report highlights that obesity levels are closely tied to social and economic conditions and that individuals with lower incomes are more at risk. People of color, who are more likely to live in neighborhoods with few options for healthy foods and physical activity, and, are the target of widespread marketing of unhealthy foods, are at elevated risk.
As of 2015-2016, the latest available data, nearly half of Latino (47 percent) and Black adults (46.8) had obesity while adult obesity rates among White and Asian adults were 37.9 percent and 12.7 percent respectively. Incidence of childhood obesity was highest amongst Latino children at 25.8 percent while 22 percent of Black children had obesity, 14 percent of White children had obesity and 11 percent of Asian children had obesity.
What Could Work?
While the obesity rates are alarming, there are new data offering the promise of policies that combat the epidemic, namely promoting healthier food for children through revamped WIC food packages and fostering behavior change through taxes on sugary drinks.
- Obesity rates for children enrolled in WIC (Special Supplemental Nutrition Program for Women, Infants and Children) continue to decline, from 15.9 percent in 2010 to 13.9 percent in 2016. In 2009, the USDA updated WIC food packages to more closely meet recommended national dietary guidelines including the addition of more fruits, vegetables and whole grains and reduced fat levels in milk and infant formula. A Los Angeles County study published this year found that 4-year-olds who had received the revised WIC food package since birth had reduced risk for obesity.
- A number of U.S. cities and the Navajo Nation have passed local taxes on sugary drinks that are showing promise as a means to change consumers’ beverage habits. Studies of a 1-cent per ounce tax in Berkeley, California and a 1.5 cent per ounce tax in Philadelphia, Pennsylvania found that the consumption of sugary drinks decreased significantly after the tax was imposed.
“Policies such as these are proving effective in changing behavior. But, no single solution – however promising – is sufficient. Obesity is a complex problem and will need multi-sector, multi-factor solutions,” said TFAH’s Auerbach.
“Creating the conditions that allow people to more easily make healthy choices is central to preventing obesity, as is prioritizing investment in those communities most affected by the crisis,” Auerbach said.
Recommendations for Policy Action
The report includes 31 recommendations for policy action by federal, state and local government, across several sectors, designed to improve access to nutritious foods and provide safe opportunities for physical activity, while minimizing harmful marketing and advertising tactics.
Among the report’s recommendations for policies to address the obesity crisis are:
- Expand the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) to age 6 for children and for two years postpartum for mothers and fully fund the WIC breastfeeding Peer Counseling Program.
- Increase the price of sugary drinks through excise taxes and use the revenue to address health and socioeconomic disparities.
- Ensure that CDC has enough funding to grant every state appropriate funding to implement evidence-based obesity prevention strategies (currently, CDC only has enough funding to work with 16 states).
- Make it more difficult to market unhealthy food to children by ending federal tax loopholes and business costs deductions related to the advertising of such foods to young audiences.
- Fully fund the Student Support and Academic Enrichment program and other federal programs that support student physical education.
- Encourage safe physical activity by funding Safe Routes to Schools (SRTS), Complete Streets, Vision Zero and other pedestrian safety initiatives through federal transportation and infrastructure funding.
- Ensure that anti-hunger and nutrition-assistance programs, like the Supplemental Nutrition Assistance Program (SNAP), WIC, and others follow the Dietary Guidelines for Americans and make access to nutritious food a core program tenet.
- Strengthen and expand school nutrition programs beyond federal standards to include universal meals, flexible breakfasts and eliminate all unhealthy food marketing to students.
- Enforce existing laws that direct most health insurers to cover obesity-related preventive services at no-cost sharing to patients.
- Cover evidence-based comprehensive pediatric weight management programs and services in Medicaid.
State by State rates of adult obesity – highest to lowest
Tie: Mississippi and West Virginia (39.5%), 3. Arkansas (37.1%), 4. Louisiana (36.8%), 5. Kentucky (36.6%), 6. Alabama (36.2%), 7. Iowa (35.3%), 8. North Dakota (35.1%), 9. Missouri, (35.0%), 10. – Tie: Oklahoma and Texas (34.8%), 12. – Tie: Kansas and Tennessee (34.4%), 14. South Carolina (34.3 %), 15. – Tie: Indiana and Nebraska (34.1%), 17. Ohio (34.0%), 18. Delaware (33.5%), 19 – Tie: Michigan, North Carolina (33.0), 21. Georgia (32.5%), 22. New Mexico (32.3%), 23. Wisconsin (32.0%), 24. Illinois (31.8%), 25. – Tie: Maryland and Pennsylvania (30.9%), 27. Florida (30.7%), 28 – Tie: Maine and Virginia (30.4%), 30. Tie: Minnesota and South Dakota (30.1%), 32. Oregon (29.9 %), 33. New Hampshire (29.6%), 34. Three-way Tie: Alaska, Arizona and Nevada (29.5%), 37. Wyoming (29.0%), 38. Washington (28.7%), 39. Idaho (28.4%), 40. Utah (27.8%), 41. Rhode Island (27.7%), 42. New York (27.6%), 43. Vermont (27.5%), 44. Connecticut (27.4%), 45. Montana (26.9%), 46. California (25.8%), 47. – Tie: Massachusetts and New Jersey (25.7%), 49. Hawaii (24.9%), 50. District of Columbia (24.7%), 51. Colorado (23.0%).
# # #
Trust for America’s Health is a nonprofit, nonpartisan organization that promotes optimal health for every person and community and makes the prevention of illness and injury a national priority. www.tfah.org. Twitter: @healthyamerica1
Tasas de obesidad en Estados Unidos con altos récords históricos
Nueve estados alcanzan tasas de obesidad en adultos superiores al 35 por ciento
El Reporte demanda por Impuestos para las Bebidas Azucaradas, Programas Ampliados de Apoyo Nutricional SNAP y WIC y un entorno que fomente la actividad física para ayudar a abordar la crisis de salud
(Washington, DC) – 12 de septiembre de 2019 – Nueve estados de EE. UU. Tenían tasas de obesidad en adultos superiores al 35 por ciento en 2018, en comparación con siete estados en ese nivel en 2017, un nivel histórico de obesidad en los EE. UU., Según el 16 ° Estado anual de Obesidad: mejores políticas para un informe más saludable de América publicado hoy por el Trust for America’s Health (TFAH).
El informe basado en parte en datos recientemente publicados del Sistema de Vigilancia del Factor de Riesgo del Comportamiento (BRFSS, por su sigla en ingles) de los Centros para el Control y la Prevención de Enfermedades, y el análisis realizado por TFAH, proporciona las tasas de obesidad anuales en todo el país. La serie El estado de la obesidad y este informe fueron posibles gracias a el financiamiento de la Fundación Robert Wood Johnson.
La obesidad tiene graves consecuencias para la salud, incluido un mayor riesgo de diabetes tipo 2, presión arterial alta, accidente cerebrovascular y muchos tipos de cáncer. Se estima que la obesidad aumenta el gasto nacional en atención médica en $ 149 billones anuales (aproximadamente la mitad de lo cual es pagado por Medicare y Medicaid) y el sobrepeso y la obesidad es la razón más común por la que los adultos jóvenes no son elegibles para el servicio militar.
Las tasas de obesidad varían considerablemente entre los estados, con Mississippi y West Virginia con el nivel más alto de obesidad en adultos en la nación con 39.5 por ciento y Colorado con la tasa más baja con 23.0 por ciento.
Por primera vez, las tasas de obesidad en adultos superaron el 35 por ciento en nueve estados en 2018: Alabama, Arkansas, Iowa, Kentucky, Louisiana, Mississippi, Missouri, Dakota del Norte y Virginia Occidental.
No muy lejos atrás en el 2012, ningún estado tenía una tasa de obesidad en adultos superior al 35 por ciento y en los últimos cinco años (2013 y 2018) 33 estados tuvieron incrementos estadísticamente significativos en sus tasas de obesidad en adultos.
“Estos últimos datos indican que nuestra crisis nacional de obesidad está empeorando”, dijo John Auerbach, presidente y director ejecutivo de Trust for America’s Health. “Nos dicen que casi 50 años después de la curva ascendente de las tasas de obesidad todavía no hemos encontrado la combinación correcta de programas para detener la epidemia”. Los programas aislados y los llamados a cambios en el estilo de vida no son suficientes. En cambio, nuestro informe destaca los cambios fundamentales que se necesitan en las condiciones sociales y económicas que hacen que sea difícil para las personas comer alimentos saludables y hacer suficiente ejercicio “.
Impacto diferencial entre las poblaciones minoritarias
El informe destaca que los niveles de obesidad están estrechamente vinculados a las condiciones socioeconómicas. Las personas con ingresos más bajos están más en riesgo. Las comunidades de color, que tienen más probabilidades de vivir en vecindarios con pocas opciones de alimentos saludables y actividad física, y que a menudo son el objetivo de una comercialización generalizada de alimentos poco saludables, también tienen un riesgo elevado.
A partir de 2015-2016, casi la mitad de los adultos latinos (47 por ciento) y los adultos negros (46.8) tenían obesidad, mientras que las tasas de obesidad entre adultos blancos y asiáticos fueron de 37.9 por ciento y 12.7 por ciento respectivamente. La incidencia de obesidad también fue más alta entre los niños latinos con un 25.8 por ciento, mientras que el 22 por ciento de los niños negros tienen obesidad, el 14 por ciento de los niños blancos tienen obesidad y el 11 por ciento de los niños asiáticos tienen obesidad.
¿Qué podría funcionar?
Si bien las tasas de obesidad son alarmantes, hay nuevos datos que ofrecen la promesa de políticas que combaten la obesidad, como promover alimentos más saludables para los niños a través de paquetes de alimentos renovados de WIC y fomentar el cambio de comportamiento a través de impuestos sobre las bebidas azucaradas.
- Las tasas de obesidad para los niños inscritos en WIC (Programa Especial de Nutrición Suplementaria para Mujeres, Bebés y Niños) continúa disminuyendo, de 15.9 por ciento en 2010 a 13.9 por ciento en 2016. En 2009, el Departamento de Agricultura de los Estados Unidos (USDA, por su siglas en inglés) actualizó los paquetes de alimentos de WIC para cumplir más estrechamente con las recomendaciones nacionales. pautas dietéticas que incluyen la adición de más frutas, verduras y granos integrales y niveles reducidos de grasa en la leche y la fórmula infantil. Un estudio del condado de Los Ángeles publicado este año encontró que los niños de 4 años que habían recibido el paquete de alimentos WIC revisado desde su nacimiento habían reducido los riegos de padecer obesidad.
- Varias ciudades de EE. UU. Y la Nación Navajo han aprobado impuestos locales sobre las bebidas azucaradas que se muestran prometedoras como un medio para cambiar los hábitos de bebidas de los consumidores. Los estudios de un impuesto de 1 centavo por onza en Berkeley, California y un impuesto de 1,5 centavos por onza en Filadelfia, Pensilvania, encontraron que el consumo de bebidas azucaradas disminuyó significativamente después de la imposición del impuesto.
“Políticas como estas están demostrando ser efectivas para cambiar el comportamiento. Pero, ninguna solución única, por prometedora que sea, es suficiente. La obesidad es un problema complejo y necesitará soluciones multisectoriales y multifactoriales “, dijo Auerbach de TFAH.
“Crear las condiciones que permitan a las personas tomar decisiones saludables con mayor facilidad es fundamental para prevenir la obesidad, al igual que priorizar la inversión en las comunidades más afectadas por la crisis”, dijo Auerbach.
Recomendaciones para la acción política
El informe incluye 31 recomendaciones para la acción política del gobierno federal, estatal y local, en varios sectores, diseñado para mejorar el acceso a alimentos nutritivos y proporcionar oportunidades seguras para la actividad física, al tiempo que minimiza las tácticas perjudiciales de marketing y publicidad.
Entre las recomendaciones del informe para las políticas para abordar la crisis de obesidad están:
- Ampliar el Programa Especial de Nutrición Suplementaria para Mujeres, Bebés y Niños (WIC) a los 6 años para niños y durante dos años después del parto para las madres y financiar completamente el Programa de Orientación de Pares de WIC para la lactancia materna.
- Aumentar el precio de las bebidas azucaradas mediante impuestos especiales y utilizar los ingresos para abordar las disparidades socioeconómicas y de salud.
- Asegurarse de que los CDC tengan los recursos suficientes para otorgar a cada estado fondos apropiados para implementar estrategias de prevención de la obesidad basadas en evidencia (actualmente, los CDC solo tienen fondos suficientes para trabajar con 16 estados).
- Hacer que sea más difícil comercializar alimentos no saludables para los niños al poner fin a los vacíos fiscales federales y las deducciones de costos comerciales relacionados con la publicidad de dichos alimentos para el público joven.
- Financiar completamente el programa de Apoyo al Estudiante y Enriquecimiento Académico y otros programas federales que apoyan la educación física del estudiante.
- Fomentar la actividad física segura mediante la financiación de Rutas Seguras a las Escuelas (SRTS), Complete Streets, Vision Zero y otras iniciativas de seguridad para peatones a través de fondos federales de infraestructura y transporte.
- Asegurar de que los programas contra el hambre y la asistencia nutricional, como el Programa de Nutrición Suplementaria (SNAP), WIC y otros, sigan las Pautas dietéticas para estadounidenses y hagan del acceso a alimentos nutritivos un principio básico del programa.
- Fortalecer y expandir los programas de nutrición escolar más allá de los estándares federales para incluir comidas universales, desayunos flexibles y eliminar todo el mercadeo de alimentos poco saludables para los estudiantes.
- Hacer cumplir las leyes existentes que ordenan a la mayoría de las aseguradoras de salud que cubran los servicios preventivos relacionados con la obesidad sin costo compartido para los pacientes.
- Cubrir el manejo del programa integral del peso pediátrico basado en evidencia y servicios en Medicaid.
Tasas de obesidad adulta por estado, de mayor a menor:
1. (Empatados): Mississippi and Virginia Occidental (39.5%), Arkansas (37.1%), 4. Louisiana (36.8%), 5. Kentucky (36.6%), 6. Alabama (36.2%), 7. Iowa (35.3%), 8. Dakota del Norte (35.1%), 9. Missouri, (35.0%), 10. – Empatados: Oklahoma and Texas (34.8%), 12. – Empatados: Kansas and Tennessee (34.4%), 14. Carolina del Sur (34.3 %), 15. – : Indiana and Nebraska (34.1%), 17. Ohio (34.0%), 18. Delaware (33.5%), 19 – Empatados: Michigan, Carolina del Norte (33.0), 21. Georgia (32.5%), 22. Nuevo Mexico (32.3%), 23. Wisconsin (32.0%), 24. Illinois (31.8%), 25. – Empatados: Maryland and Pennsylvania (30.9%), 27. Florida (30.7%), 28 – Empatados: Maine and Virginia (30.4%), 30. Empatados: Minnesota and Dakota del Sur (30.1%), 32. Oregon (29.9 %), 33. New Hampshire (29.6%), 34. Empatados: Alaska, Arizona and Nevada (29.5%), 37. Wyoming (29.0%), 38. Washington (28.7%), 39. Idaho (28.4%), 40. Utah (27.8%), 41. Rhode Island (27.7%), 42. Nueva York (27.6%), 43. Vermont (27.5%), 44. Connecticut (27.4%), 45. Montana (26.9%), 46. California (25.8%), 47. – Empatados: Massachusetts and Nueva Jersey (25.7%), 49. Hawaii (24.9%), 50. Districto de Columbia (24.7%), 51. Colorado (23.0%).
# # #
Trust for America’s Health es una organización sin fines de lucro y no partidista que promueve la salud óptima para cada persona y comunidad y hace de la prevención de enfermedades una prioridad nacional. WWW.tfah.org
U.S. Obesity Rates Reach Historic Highs – Racial, Ethnic, Gender and Geographic Disparities Continue to Persist

Vaccines Prevent Infectious Disease Outbreaks and Protect Communities (August 2019)
Infectious diseases disrupt the lives millions of Americans every year. Fortunately, vaccines can prevent many of these diseases. Nonetheless, because the U.S. vaccination rates are lower than they should be, unnecessary illness and even death occurs.
For example, the seasonal flu causes much preventable suffering. The Centers for Disease Control and Prevention (CDC) found an estimated 80,000 people died—among them, 185 children—from seasonal flu in 2017–2018, nearly twice what is considered typical during an average flu year. In addition to the devastating health impacts, it is estimated that seasonal flu costs the nation approximately $87 billion in medical spending and lost work productivity annually.
The U.S. is currently in the midst of its worst measles outbreak in two decades, causing more than 1,000 cases. With the measles outbreak still growing, it is important to highlight the life-saving impacts of vaccines for people of all ages and take actions to ensure that vaccine use remains a common practice.
Key Findings
- Vaccines have helped save up to 3 million lives per year worldwide by preventing diseases such as hepatitis B, meningitis, measles and polio. Additionally, researchers say that every dollar spent on vaccination brings back return on investment in health, economic and societal benefits in 94 low to middle income countries.
- The CDC estimates that vaccination of children born between 1994 and 2018 in the U.S. will prevent 419 million illnesses, help avoid 936,000 deaths, and save nearly $1.9 trillion in total societal costs.
- In 2018, the CDC reported that the percentage of children under age 2 who had not received any recommended vaccinations quadrupled since 2001.
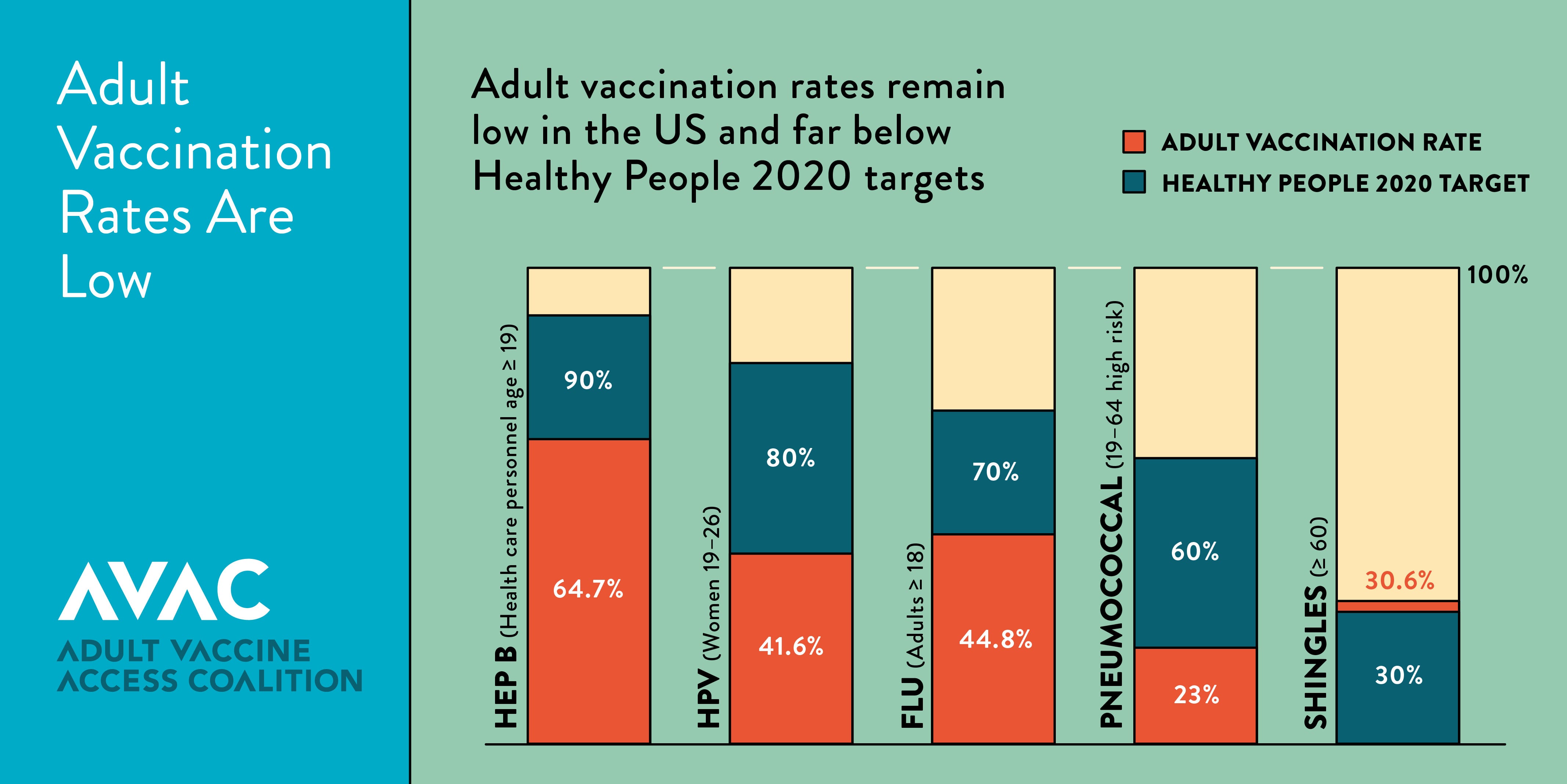
- Adult vaccination rates remain far below targets in Healthy People 2020, including for hepatitis B, seasonal flu, pneumococcal, and shingles.
- Seasonal flu vaccination rates for Americans ages 6 months and older dropped from 47 percent in the 2016-2017 season to 42 percent during the 2017-2018 season. The 2017– 2018 flu season in the United States was the deadliest in nearly 40 years—tragically underscoring the importance of annual vaccination.
- The World Health Organization has named vaccine hesitancy, the reluctance or refusal to vaccinate despite the availability of vaccines, as one of the top ten threats to global health.
Recommendations
- Significantly increase support for the vaccine infrastructure, outbreak prevention and response. CDC’s immunization program supports state and local immunization programs to increase vaccine rates among uninsured and underinsured adults and children, respond to outbreaks, educate the public and target hard-to-reach populations, improve vaccine confidence, establish partnerships, and improve information systems. Funding has not kept up with needs as states have to spend immunization dollars to respond to outbreaks, increases in the numbers of those who lack health insurance and vaccines, such as HPV, that are underused. Congress should significantly increase funding for CDC’s immunization program.
- Raise awareness about the importance of vaccination and improve vaccine acceptance. Government, healthcare providers, health systems and other trusted partners should use varied and targeted media channels to educate people about the importance, effectiveness, and safety of vaccinations. Congress should provide needed resources to the United States Department of Health and Human Services to study the causes for vaccine resistance and to educate clinical providers on methods for improving vaccine acceptance.
- Minimize vaccine exemptions for schoolchildren and healthcare workers. States should enact policies that enable universal childhood vaccinations to ensure children, their classmates, educators and the general public are protected from vaccine-preventable diseases. This includes eliminating non-medical exemptions and opposing legislation to expand exemptions. States should ensure medical vaccine exemptions are only given when appropriate and are not used as a de facto personal belief exemption in states where those exemptions have been eliminated. Healthcare personnel should also be required to receive all recommended vaccinations of the Advisory Committee on Immunization Practices (ACIP) in order to protect staff and patients, assure continuity of operations in the event of an outbreak and, achieve necessary healthcare infection control. Healthcare facilities should ensure access to vaccines for all staff and contractors and remove barriers for staff receiving vaccines.
- Ensure first-dollar coverage for recommended vaccines under Medicaid, Medicare, and commercial insurance. Public and private payers should ensure that ACIP-recommended vaccines are fully covered, as cost-sharing can be a significant barrier to vaccination.
- Increase the pool of providers who immunize. As new vaccines are approved, reaching target populations will be critical. States can expand certain health care providers’ roles and scopes of practice to increase the pool of professionals who give shots, such as pharmacists and paramedics. All insurance plans should consider including pharmacies and other complementary providers as in-network and receive equal payment for vaccine administration services for their adult and pediatric populations.
Prevention and Public Health Fund State Fact Sheets
3 WINS Fitness: Free Exercise Classes get Communities Moving

{kind=link}
Regular physical activity promotes good health and well-being. Yet, about 80 percent of American adults do not meet the minimum recommended levels for cardiovascular activity and strength training needed to support optimal health and prevent the risk of chronic diseases.
3 WINS Fitness seeks to improve community health by increasing people’s physical activity levels. Launched in 2011 as 100 Citizens by California State University, Northridge’s (CSUN) Department of Kinesiology in partnership with Recreation Park in San Fernando, CA, 3 WINS Fitness offers a tailored and comprehensive free exercise intervention that is sustainable and replicable through its delivery by university kinesiology students. Programs are provided at public parks, faith-based institutions, and public schools, and currently they operate at six sites across Los Angeles County serving over 300 participants.
In 2013 the White House recognized and gave an award to the program through First Lady Michelle Obama’s “Let’s Move!” campaign. Since then, the program has scaled to three other universities within the California State University system.
Their program’s “3 WINS” reflects their social impact priorities: community health, participant fitness, and student professional development.
WIN 1: Community Health
Access and affordability to safe places to engage in physical activity promotes optimal community health. However, many low-income communities do not have affordable access to safe places for physical activity, and thus have a disproportionate burden of disease compared to wealthier communities.
Steven Loy, Ph.D., professor of kinesiology at CSUN and founder/faculty advisor for 3 WINS Fitness says the program focuses on those underserved communities which are at high risk for diabetes, cardiovascular disease, obesity and other chronic diseases related to physical inactivity.
“Having a program in their neighborhood park, school, and church where they can easily walk to and exercise, especially where there are no other physical activity programs is important,” said Loy. “We are holding it in communities that county public health has identified as areas where health inequities exist, and we are helping to address the social determinants of health by improving the physical activity conditions of those communities.”
Loy says through their research with RAND Corporation and the data they have collected, they observed a greater use of park facilities with the introduction of structured physical activity, in particular for the senior population reflecting a sense of safety and community among themselves and their students.
WIN 2: Participant Health

3 WINS Fitness provides participants with a dynamic 60-minute exercise routine three times per week for adults of all ages and fitness abilities, including a falls prevention group, and free diabetes prevention program modified from the National Diabetes Prevention Program.
Loy noted, “participants who attend the three classes per week exceed the minimum recommended levels for cardiovascular activity and strength training cited in the 2018 Physical Activity Guidelines. Throughout the years, our 3 WINS Fitness participants have had many success stories.”
“Doctors said I would need surgery for a back injury, I was in constant pain, I couldn’t even lift my arms to brush my hair” said 3 WINS participant of two years Balvina Nuño. “Since joining 3 WINS, the injury has healed without surgery. I can now lift my arms over my head, and I have lost 30 pounds! I am thankful to God and the instructors for giving me my life back.”
Other participants of the program have also reported improved health.
“I started 3 WINS Fitness last summer and have lost over 40 pounds,” said Andrea Veronica. “I am diabetic and was required to inject insulin 6 times a day. Because of this program, today I am no longer required to inject myself or take any medication. I am happy and feel more energetic than ever!”
“I started this program in October 2017 as a pre-diabetic,” added Candy Lopez. “I have lost 24 pounds, and I feel happier and have more energy. I love coming here because the participants and instructors create such a strong family-like community that I feel motivated to come workout every time.”
WIN 3: Student Professional Development
The kinesiology students involved in the program include both undergraduate and graduate students trained and educated in exercise and human movement. For them, 3 WINS Fitness is an opportunity to apply their education, gain job-related experience, and grow in leadership skills and self-empowerment.
“Noting the constant changes happening in health care reform, I realized what we are doing through 3 WINS Fitness is so special and is soon, if not already, to become the face of preventative health care methods that is efficient, cost-effective, and helps not only me as a healthcare provider, but most importantly, the individuals in the communities around us attain their best level of health and fitness,” said Angelica Alberto, a former 3 WINS Fitness student volunteer who is now pursuing a Doctor of Physical Therapy and Master of Public Health dual degree at Northwestern University.
Loy says it is also an opportunity to show communities what those educated in kinesiology can do for public health.
“We have found that there are few opportunities created for kinesiology and public health to work together. We are trying to change that with upstream solutions to the ideas promoted by Public Health 3.0,” said Loy. “We have recruited students to create an ongoing army of individuals trained in physical activity who are pursuing additional public health education opportunities, and, are motivated and enthusiastic to deliver programming that reaches the whole community to improve health.”
Where is the Program Going?

3 WINS Fitness participants receive exercise programming from 3 WINS Fitness kinesiology students during a 3 WINS
Fitness Summit held in April 2018.
Throughout 3 WINS Fitness’ journey, partnerships have been critical. The program has teamed with public and private sector partnerships with parks and recreation, public health, universities and research institutions, hospitals, and health and fitness organizations to sustain, scale, and provide accessible physical activity programming to communities.
One of those partners is the American Council on Exercise (ACE). Cedric Bryant, Ph.D., ACE President and Chief Science Officer says “ACE’s partnership with 3 WINS Fitness helps us fulfill our mission to get people moving, regardless of age, gender, race, or socioeconomic background.”
In the spring of 2018, ACE partnered with 3 WIN Fitness to hold a Summit to demonstrate the program to stakeholders. One of the attendees included Loretta DiPietro, Ph.D., professor of exercise and nutrition sciences at the Milken Institute School of Public Health at George Washington University in Washington, D.C. She was also a committee member of the 2018 Physical Activity Guidelines Advisory Committee which reviewed the scientific evidence and prepared a report about physical activity and health for the second edition of the Physical Activity Guidelines for Americans.
She said, “I’ve been waiting my entire public health career to see the science of exercise and physical activity translated and scaled up to the community level so elegantly and effectively. The cultural wave of change in how communities adopt an active lifestyle begins now with 3WINS Fitness!”
According to a study done by the Centers for Disease Control and Prevention, 11.1 percent in total health care expenditures were associated with inadequate levels of physical activity. However, if programs were in place to help adults meet current guidelines for physical activity, the country could avert up to an estimated $117 billion in preventable health care spending.
Loy said 3 WINS Fitness is part of that solution, and their next goal is to scale 3 WINS Fitness through universities across the country by training staff to develop and sustain their own program specific to their community.
“There are over 700 universities with kinesiology programs,” said Loy. “Our experience in replicating our program, as well as scaling it to other universities has identified the challenges existing for collaboration among public health, kinesiology, parks and recreation, and faith-based organizations, but it has also been an 8-year demonstration that an affordable sustainable solution is possible if we work together. The university kinesiology model can drive community wide disease prevention programs which can be customized for the needs of the community.”
*3 WINS Fitness Banner Photo Credit: Carmen Anthony